Familial Autosomal Polyposis (FAP)
Presentation :
- Numerous polyps throughout the colon and rectum, often developing in early teens w/ nearly 100% lifetime risk of colorectal cancer by age 40 if untreated
- May also develop desmoid tumors, duodenal or ampulla of Vater adenocarcinoma, among other cancers
- About 30% of individuals with FAP have no known family history and represent de novo APC mutations
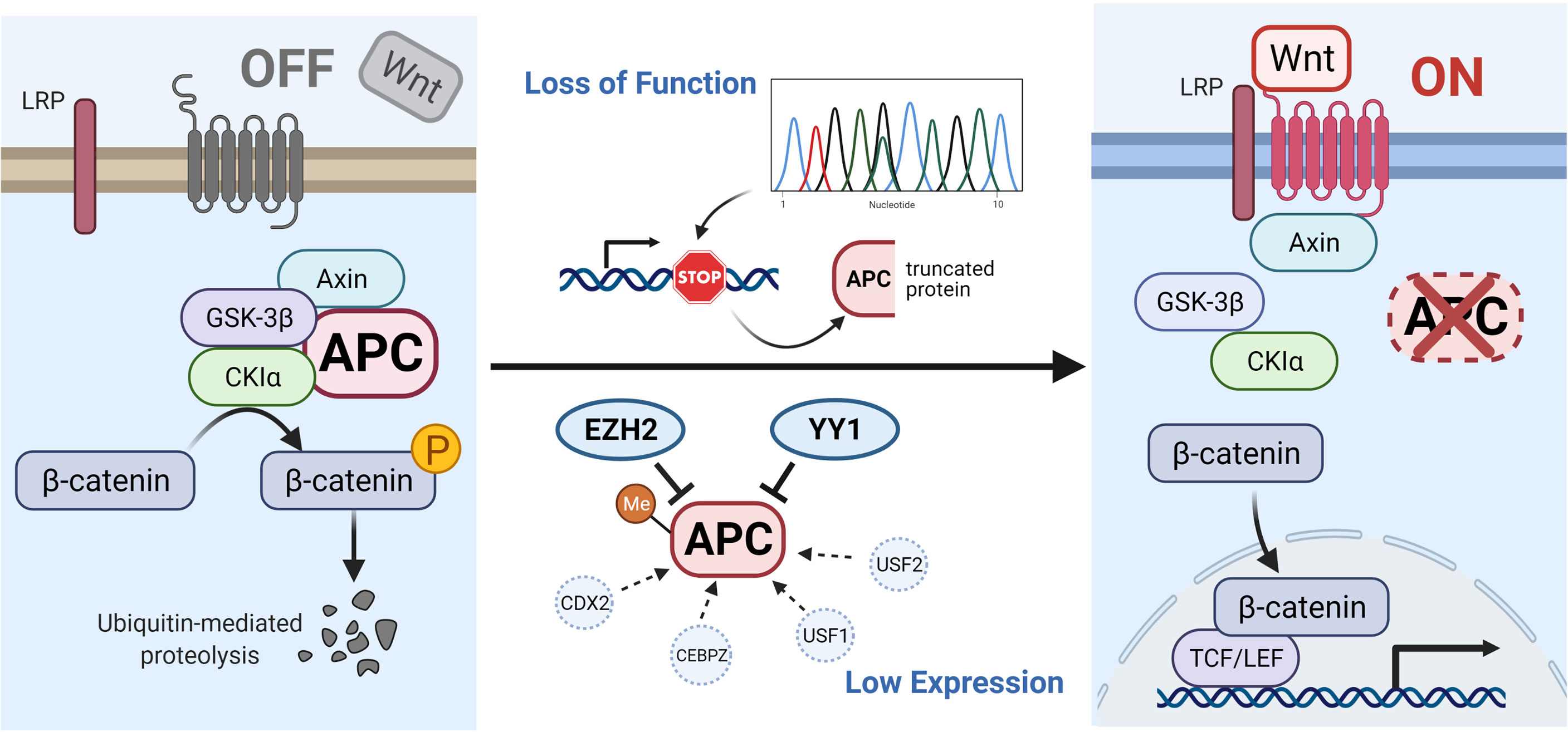
Pathophysiology :
- Mutations to the APC (adenomatous polyposis coli) gene leading to failure of beta-catenin degradation. Beta-catenin can then enter the nucleus leading to uncontrolled cell replication.
Diagnostic Testing:
- Patients with known FAP or a strong family history FAP should undergo annual endoscopy evaluation with flexible sigmoidoscopy or colonoscopy starting at 10 to 12 years of age.
- Surveillance should continue until the polyp load is unable to be controlled with endoscopic removal
Treatment :
- Definitive management involves colectomy +/- proctectomy
- If the rectum is left intact, endoscopic surveillance must be performed every six months as the risk of developing rectal cancer is as high as 29% at 50 years of age. Candidates for rectal sparing include those with a low polyp burden within the rectum, lack of advanced rectal neoplasia, and no evidence of CRC at the time of resection. For appropriately selected patients, the conversion to total proctocolectomy is near zero but increases to 35% in poorly surveillance candidates
- Total proctocolectomy (TPC) involves the removal of the colon and rectum with the creation of either an ileostomy or an ileoanal pouch. Although no surveillance is required, there are disadvantages to this approach. TPC with ileoanal pouch can result in increased rates of infertility in men and women as well as urinary dysfunction. Although there is no difference in incontinence, there is an increase in stool urgency with an ileoanal pouch.
- Sulindac (NSAID) has been shown in small studies to reduce the number of adenomas by nearly 50% and the size of adenomas by 65%. For patients with a retained rectum, can reduce the polyp burden.
Prognosis:
- Untreated patients have a short life expectancy, with most dying in the 4th decade of life.
- After colectomy, pts still develop desmoid tumors and other GI cancers (primarily adenocarcinoma of the duodenum and papilla of Vater).
- Desmoid tumors in FAP patients are often aggressive and tend to locally invade, leading to compression, obstruction, and blockage of blood vessels and nerves.
References:
Created on: Tuesday 04-09-2024