Hyponatremia
Presentation :
Pathophysiology :
ADH Physiology:
- ADH is the primary hormone responsible for tonicity homeostasis
- ADH is stored in neurons within the hypothalamus which express osmoreceptors responsive to changes in serum osmolarity
- Elevations in osmolarity result in the secretion of ADH to retain water and thus normalize osms
- ADH secretion may also be caused by detection of hypovolemia by baroreceptors in L atrium, carotid artery, and aortic arch
- Signaling is via the vagus nerve, which directly stimulates the release of ADH
- ADH principally exerts its effects by binding to the kidneys principal cells within the late distal tubule and collecting ducts. ADH binds to the V receptor which ultimately phosphorylates intracellular aquaporin-2 (AQP2) storage vesicles, causing their movement and insertion into the cell membrane.
- AQP2 is a water channel that allows water to move passively into the cell guided by the osmotic gradient established by NaCl and urea, and thus promotes reabsorption of water in the kidney.
- ADH also binds to V receptors on vascular smooth muscle, causing a release of intracellular calcium from the endoplasmic reticulum and contraction of vascular smooth muscle leading to increases in total peripheral resistance and thus increases in blood pressure.
RAAS Physiology:
Diagnostic Testing:
Prior to treatment, send:
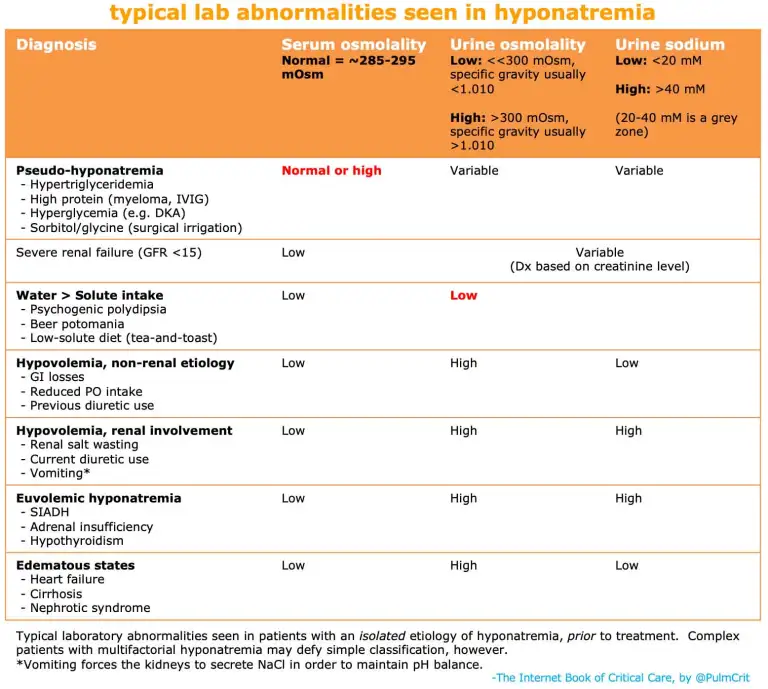
- Serum osmolality
- Urine osmolality and electrolytes (Na, Cr, and optionally Urea)
- Verify true hyponatremia by checking serum osmolality less than ~285.
- Normal or elevated serum osms suggests unmeasured solute:
- Severe hyperglycemia.
- Severe uremia
- Triglyceride level >1,500 mg/dL.
- High protein level (multiple myeloma, IVIG).
- Exogenous osmoles:
- Contrast dye.
- Mannitol administration.
- Maltose (from IVIG).
- Sorbitol/glycine (used for surgical irrigation).
- Alcohols (ethanol, methanol, etc)
- Normal or elevated serum osms suggests unmeasured solute:
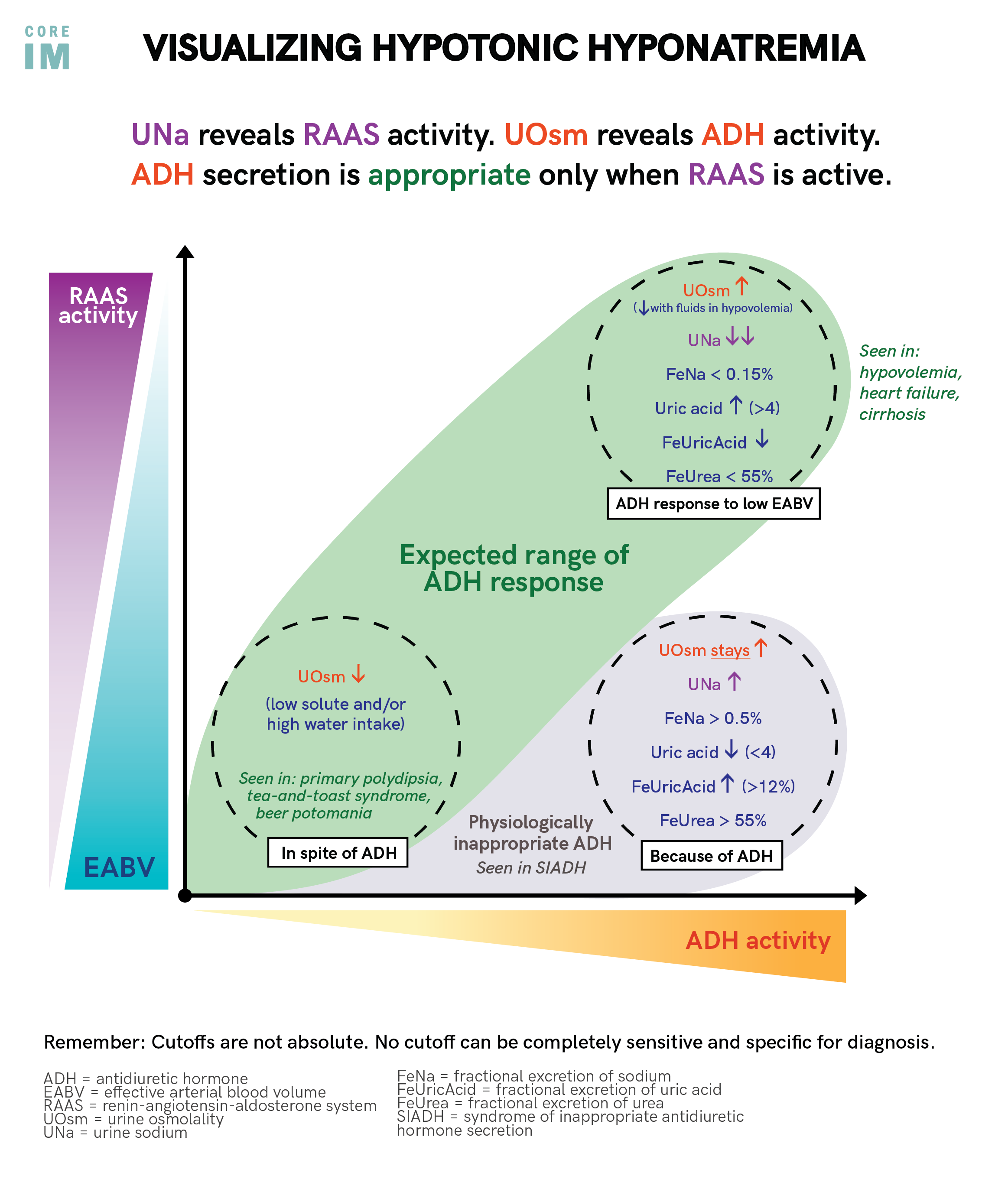
- Check urine osmolality (HIGH if >300)
- Low suggests body is detecting decreased serum osm and trying to correct by dumping water in urine
- Causes include either increased free water intake OR decreased solute intake
- Psychogenic polydipsia (free water up)
- Tea-Toast Syndrome (solute down)
- Beer Potomania (both free water up and solute down)
- Alternatively, may represent recovery phase from any other cause of hyponatremia (e.g., the patient initially had hypovolemic hyponatremia, received volume resuscitation prior to urinalysis, and is currently auto-correcting their own sodium levels.)
- Secretion of dilute urine will cause the patient's sodium to rise – so these patients may correct their own sodium levels.
- Production of large volumes of dilute urine is often a sign that the sodium is about to over-correct.
- Causes include either increased free water intake OR decreased solute intake
- High suggests body is detecting elevated serum osm and trying to correct by retaining water (OR is over-producing ADH)
- Concentrated urine indicates that the kidney is still retaining water. This indicates that the patient is not going to auto-correct their sodium.
- A very concentrated urine suggests that giving isotonic fluid could potentially worsen the hyponatremia (because the kidney may respond by retaining water and excreting sodium, a process termed “desalination”).
- Low suggests body is detecting decreased serum osm and trying to correct by dumping water in urine
- Check clinical volume status and urine Na
Treatment :
Prognosis:
Other Figures:

References:
- https://emcrit.org/ibcc/hyponatremia/
- https://www.coreimpodcast.com/2021/02/10/5-pearls-on-hyponatremia-episode-1/
- https://www.ncbi.nlm.nih.gov/books/NBK526069/
Created at: periodic/daily/August/2023-08-05-Saturday