Lyme Disease
Presentation :
- 3 Major Phases of Disease:
- Early Localized (≤4 wk):
- EM at site of tick attachment, variably with fever, lymphadenopathy, myalgia
- Erythema Migrans: usually painless, nonpruritic, and circumferentially enlarging

- Local cutaneous reactions resulting from hypersensitivity to tick saliva may resemble EM but tend to occur earlier, are pruritic, and do not enlarge significantly after onset.
- Early disseminated (2 wk-6 mo): Without treatment, hematogenous dissemination occurs in up to 60% of patients.
- Constitutional: flu-like syndrome
- Cardiac: heart block, myocarditis
- Dermatologic: Multiple sites of EM at sites distant from the original tick attachment
- Neurologic: cranial neuropathies, meningitis, radiculitis, mononeuritis multiplex, spinal cord or brain parenchymal inflammation
- Late disseminated (≥6 mo):
- Arthritis: Approximately 60% of untreated patients with Lyme disease develop a monoarticular or oligoarticular inflammatory arthritis as a late complication
- Neurologic: peripheral neuropathy, encephalopathy
- Dermatologic: acrodermatitis chronica atrophicans
- Early Localized (≤4 wk):
Pathophysiology :
- Transmitted by Ixodes scapularis (Blacklegged Deer Tick)
- The causative spirochete, Borrelia burgdorferi, is transmitted intradermally when a tick ingests a blood meal.
- Transmission typically occurs after at least 36 hours
Diagnostic Testing:
- Patients with EM and a compatible exposure history do not require confirmatory laboratory testing before treatment
- Early disseminated Lyme disease should be evaluated using ELISA followed by confirmatory testing
Treatment :
- Prophylaxis:
- In highly select situations, prophylaxis with a single dose (200 mg) of doxycycline may decrease the risk of Lyme disease after a tick bite. Prophylactic doxycycline is only recommended. Otherwise, observation is recommended, with treatment given if suggestive symptoms develop.
- the tick is reliably identified as a blacklegged deer tick
- attachment lasts 36 hours or longer
- antibiotics can be started less than 72 hours after tick removal
- prevalence of B. burgdorferi infection of ticks in the region exceeds 20%.
- In highly select situations, prophylaxis with a single dose (200 mg) of doxycycline may decrease the risk of Lyme disease after a tick bite. Prophylactic doxycycline is only recommended. Otherwise, observation is recommended, with treatment given if suggestive symptoms develop.
- Early Localized:
- Doxycycline, 100 mg PO BID × 10 d (first-line therapy)
- Amoxicillin, 500 mg PO TID × 14 d
- Cefuroxime axetil, 500 mg PO BID × 14 d
- Early Disseminated:
- Cardiac:
- Hospitalized patients (first-degree block with PR interval ≥300 msec, higher degree heart block, other arrhythmias, myopericarditis): initial IV ceftriaxone with transition to oral for total of 14-21 days
- Outpatients (first-degree AV block with PR interval <300 msec): oral treatment same as for early localized disease × 14-21 d
- Meningoencephalitis: IV penicillin G, IV cefotaxime, or IV ceftriaxone or oral doxycycline × 14-21 d (IV antibiotics preferred for spinal or brain parenchymal involvement)
- Other manifestations (including facial palsy): oral treatment the same as for early localized disease × 14-21 d
- Cardiac:
- Late Disseminated:
- Initial rheumatologic treatment: same as for early localized but × 28 d
- Arthritis unresponsive to initial treatment: IV ceftriaxone 2-4 weeks
Prognosis:
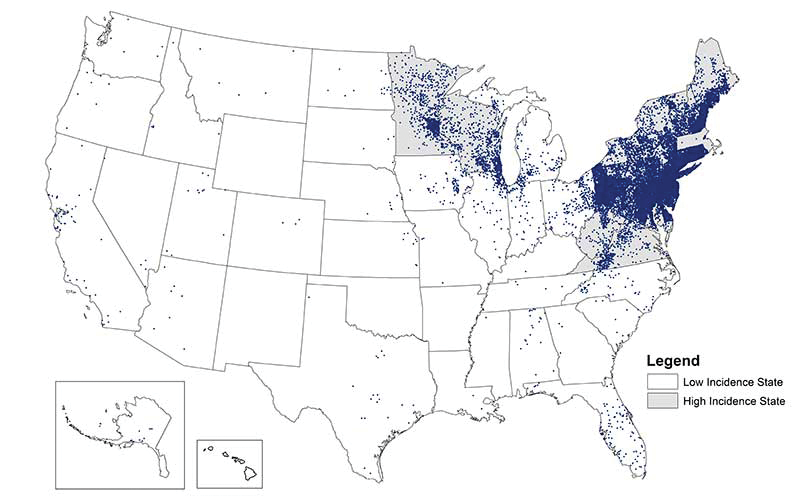
Lyme Disease Distribution
References:
- MKSAP
Created at: periodic/daily/July/2023-07-31-Monday