Presentation :
Pathophysiology :
- Approximately one half of melanomas harbor a BRAF gene mutation (most commonly V600E), and another 20% have an MEK or NRAS mutation
Diagnostics :
- Nodal metastases are uncommon in thin melanomas, and nodes are typically not assessed if the melanoma has a Breslow depth of less than 0.8 mm and is without ulceration.
- Assessing for lymph node metastasis with lymphatic mapping and sentinel lymph node biopsy is often recommended for intermediate and thicker melanomas.
- Completion lymph node dissection is no longer routinely performed, as there is no improvement in survival
Treatment :
- Localized Disease
- Surgical Margins:
- 1cm margins for lesions <1 mm thick.
- 1-2cm margin for lesions 1-2 mm thick.
- 2cm margins for lesions >2 mm thick
- Oligometastatic disease:
- In patients with one or a very limited number of metastases, surgical excision of all metastatic disease can occasionally produce durable benefit.
- Metastatic disease:
- In contrast to immunotherapy and targeted therapy, cytotoxic chemotherapy has not been shown to increase survival or to induce durable remissions
- Targeted therapy:
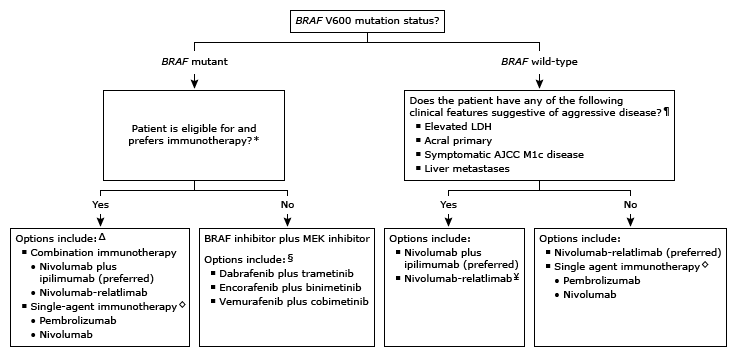
- Melanomas with BRAF V600E/V600K may respond to oral therapy with the available BRAF/MEK inhibitor combinations (dabrafenib/trametinib; vemurafenib/cobimetinib; encorafenib/binimetinib)
- Immunotherapy:
- UTD Algo:
Prognosis:
- A high mitotic rate, lymphovascular invasion, and the presence of ulceration are poor prognostic signs.