Nephrolithiasis
Presentation :
- classic symptoms are acute flank pain with radiation to the groin and hematuria
Pathophysiology :
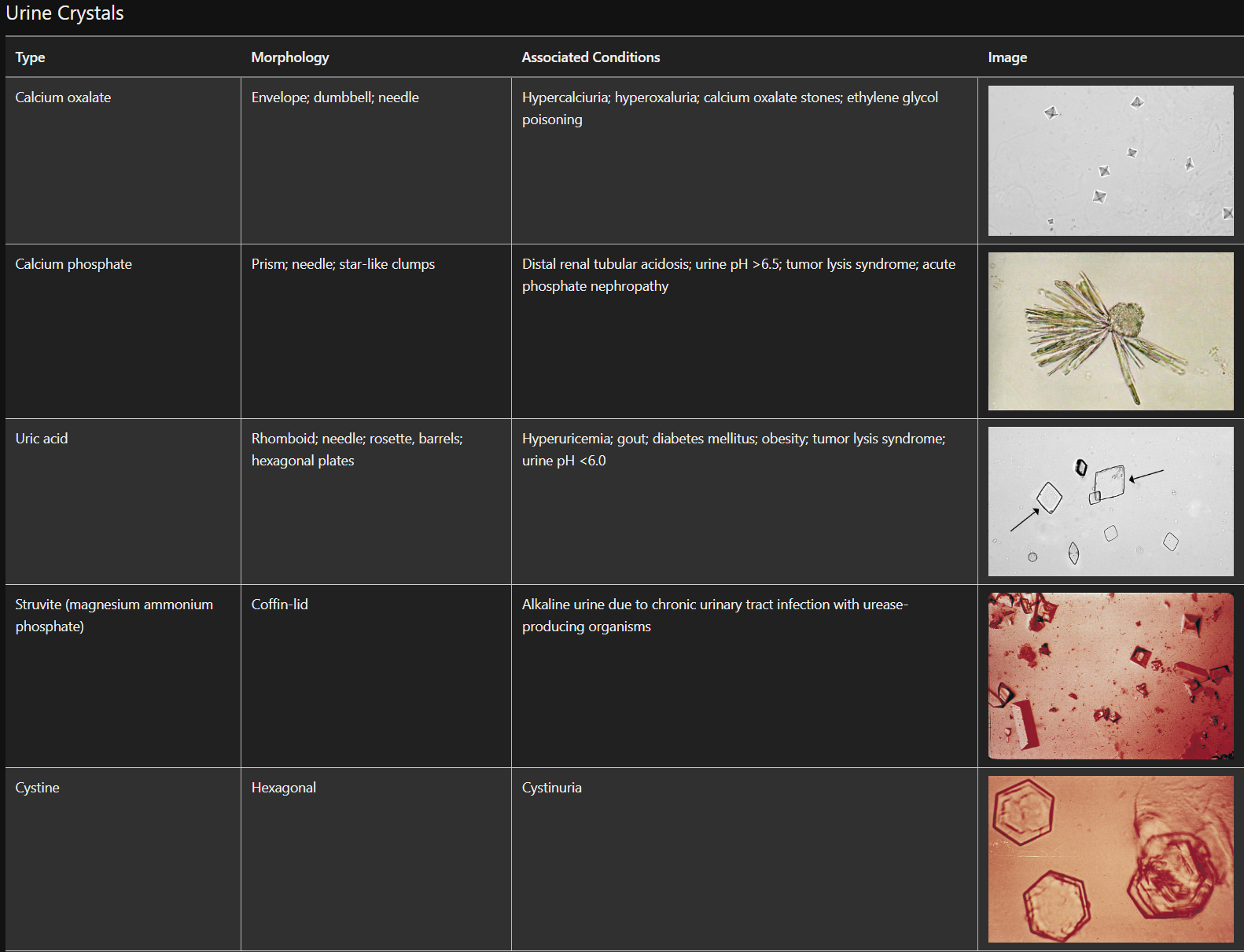
- High intake of vitamin C, which is metabolized to oxalate, can cause hyperoxaluria.
- Unless excessive, dietary calcium should not be restricted because this will increase oxalate absorption
- Because citrate prevents calcium crystal formation, low urine levels are associated with increased stone formation
Diagnostic Testing:
- Urinalysis usually reveals blood, and the urine sediment has nondysmorphic erythrocytes
- The absence of erythrocytes on urinalysis does not rule out nephrolithiasis.
- Ultrasonography (indicated during pregnancy) or noncontrast CT is the preferred imaging choice.
- Patients should strain their urine to collect stone fragments for chemical analysis if the type of stone is unknown.
- 24-hour urine collection for measurement of volume, calcium, oxalate, citrate, uric acid, and sodium should be obtained from all patients with recurrent stones
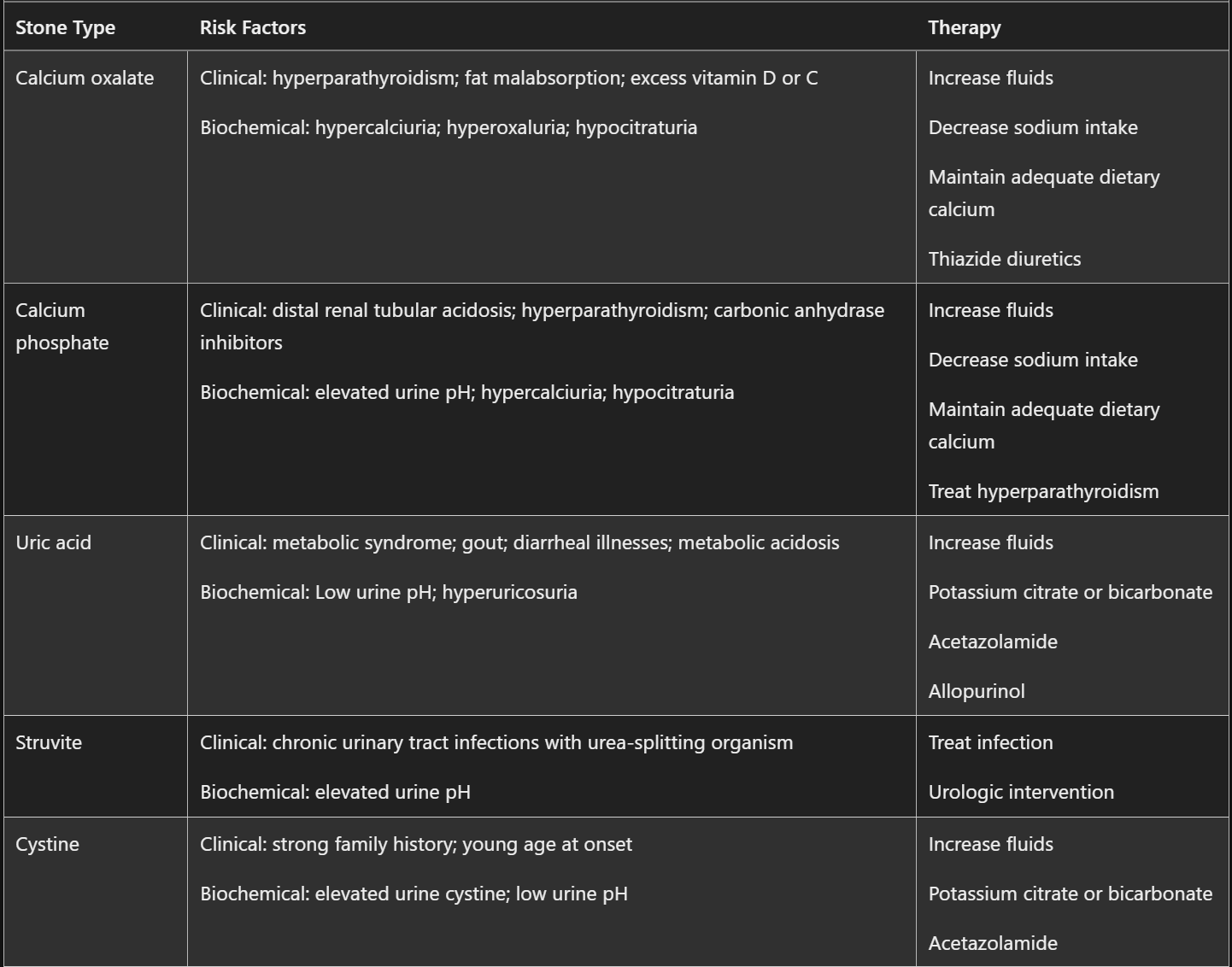
Treatment :
- Calcium stones:
- Because calcium excretion parallels sodium excretion, limiting sodium intake will also lower urine calcium
- If hypercalciuria is present, calcium excretion can be decreased by the use of thiazide diuretics
- Unless excessive, dietary calcium should not be restricted because this will increase oxalate absorption
- Urate stones:
- Alkalinizing the urine with potassium citrate or bicarbonate increases the solubility of uric acid
- Allopurinol can be beneficial if uric acid excretion is elevated.
- All stones:
- Increased fluid intake is the most important intervention to prevent recurrent disease regardless of stone composition.
- Urine output should be >2500 mL/d to decrease urine solute concentration.
- Kidney stones <5 mm in diameter typically pass spontaneously
- Stones >10 mm often require invasive treatment (shock wave lithotripsy, ureteroscopy with laser ablation, or percutaneous nephrolithotomy)
- Patients with 6- to 10-mm stones may be treated with tamsulosin, nifedipine, silodosin, and tadalafil to enhance stone expulsion, but efficacy is controversial. Because few adverse effects are attributed to these medications, they are often recommended.
- Urgent urologic consultation is indicated for patients with:
- pyelonephritis or urosepsis
- AKI
- stones >10mm requiring surgical removal
- bilateral obstruction
- obstruction of a solitary kidney
- ambulatory patients who do not pass stones with conservative management
- Low-calcium diet may actually harm. Calcium restriction does not prevent stones and may actually increase stone formation and contribute to bone demineralization.
- Increased fluid intake is the most important intervention to prevent recurrent disease regardless of stone composition.
Prognosis:
References:
Created on: Saturday 08-12-2023