Peripheral Artery Disease
Presentation :
-
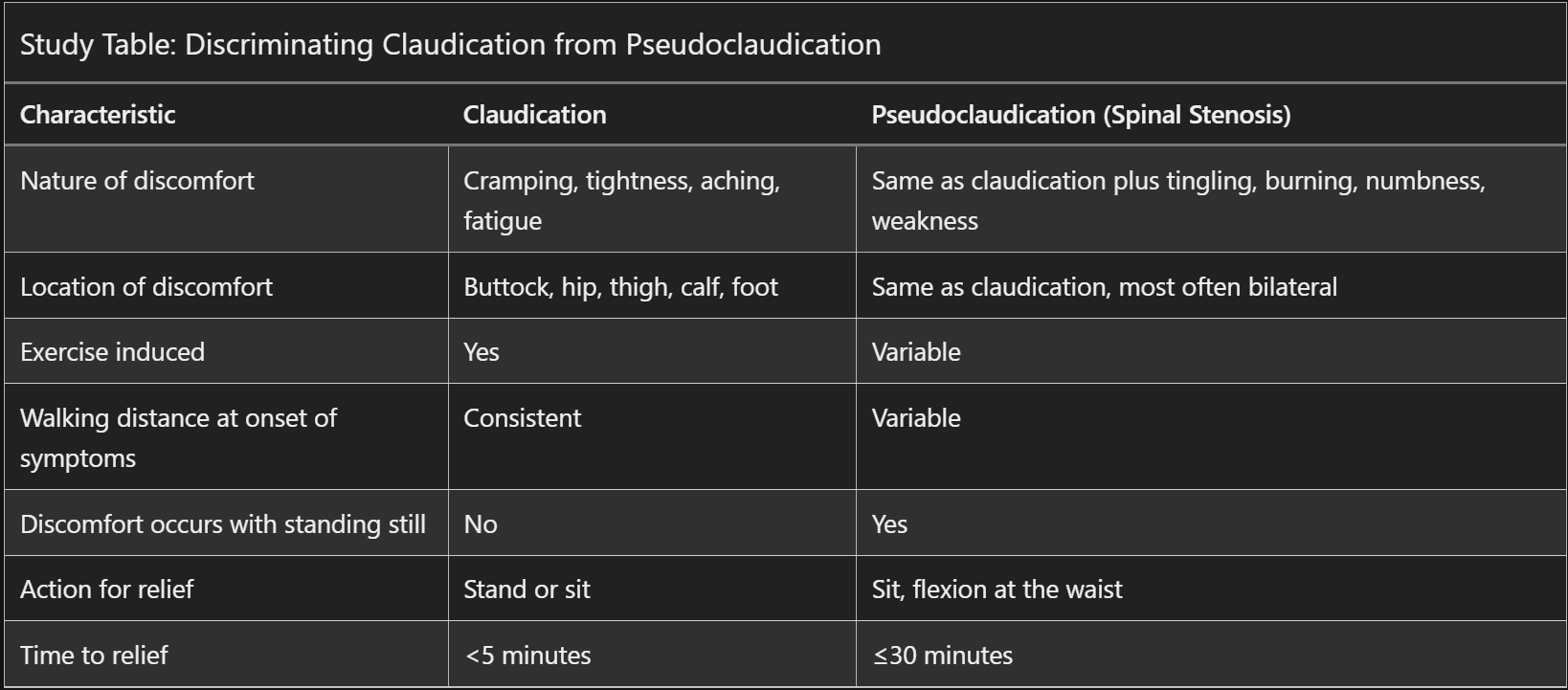
Intermittent claudication is the classic sign of PAD
-
Pathophysiology :
Diagnostic Testing:
- Resting ABI should be performed on all patients with a history or physical examination suggesting PAD
- Normal ABI is >0.9 to ≤1.40.
- ABI ≤0.90 is compatible with PAD
- For pts with ABI >1.40, this likely results from calcified, noncompressible arteries.
- These patients should proceed to toe-brachial index; <0.70 indicates PAD
- Exercise treadmill ABI testing should be performed for patients with normal or borderline resting ABI values and unexplained exertional leg symptoms
- Noninvasive angiography with duplex ultrasonography, CTA, or MRA is performed for anatomic delineation of PAD in patients requiring surgical or endovascular intervention.
Treatment :
- Exercise training is the most effective treatment for improvement in functional status in patients with PAD.
- Optimize CAD risk as per usual:
- smoking cessation
- BP goal <130/80 mm Hg
- aspirin (preferred over clopidogrel)
- moderate- or high-intensity statin therapy
- cilostazol for patients with intermittent claudication
- AVOID in patients with a low LVEF or history of HF
- PCI or surgery for patients who do not improve with medical therapy OR have pain at rest OR poorly healing ulcers.
- Patients with acute limb ischemia require heparin anticoagulation as well as urgent surgical consultation.
Prognosis:
References:
Created at: periodic/daily/August/2023-08-05-Saturday