Sweet Syndrome
AKA Acute Febrile Neutrophilic Dermatosis
Presentation :
-
Fever is almost always present
- Almost all drug-induced cases will have fever
- ~80% of maligant and classical cases will have fever
-
Rash: typically abrupt onset, erythematous/violaceous, tender/burning, edematous, and inflamed papules/plaques (significant dermal edema causes raised lesions; may also lead to pseudovesicular or pustular appearance). May have a targetoid appearance in some cases.
- Upper extremities are most commonly involved, but can be widely distributed on trunk, lower extremities, head, and neck


-
Extracutaneous symptoms:
- Constitutional sx: arthralgia, myalgia, fatigue, malaise, and headache
- Occular manifestations: inflammation, especially conjunctivitis but also episcleritis, scleritis, keratitis
- Many other uncommon manifestations in other organs
-
Three major categories of presentations:
- Classical (majority of cases): associated with IBD, pregnancy, infections (URIs, GI infxns, and others; usually 1-3wk later), and less commonly other autoimmune diseases
- Malignancy-associated: may precede, follow, or appear concurrently with a malignancy. More commonly hematologic (AML, MPNs), but solids as well.
- Occurrence in pts in remission may suggest disease recurrence
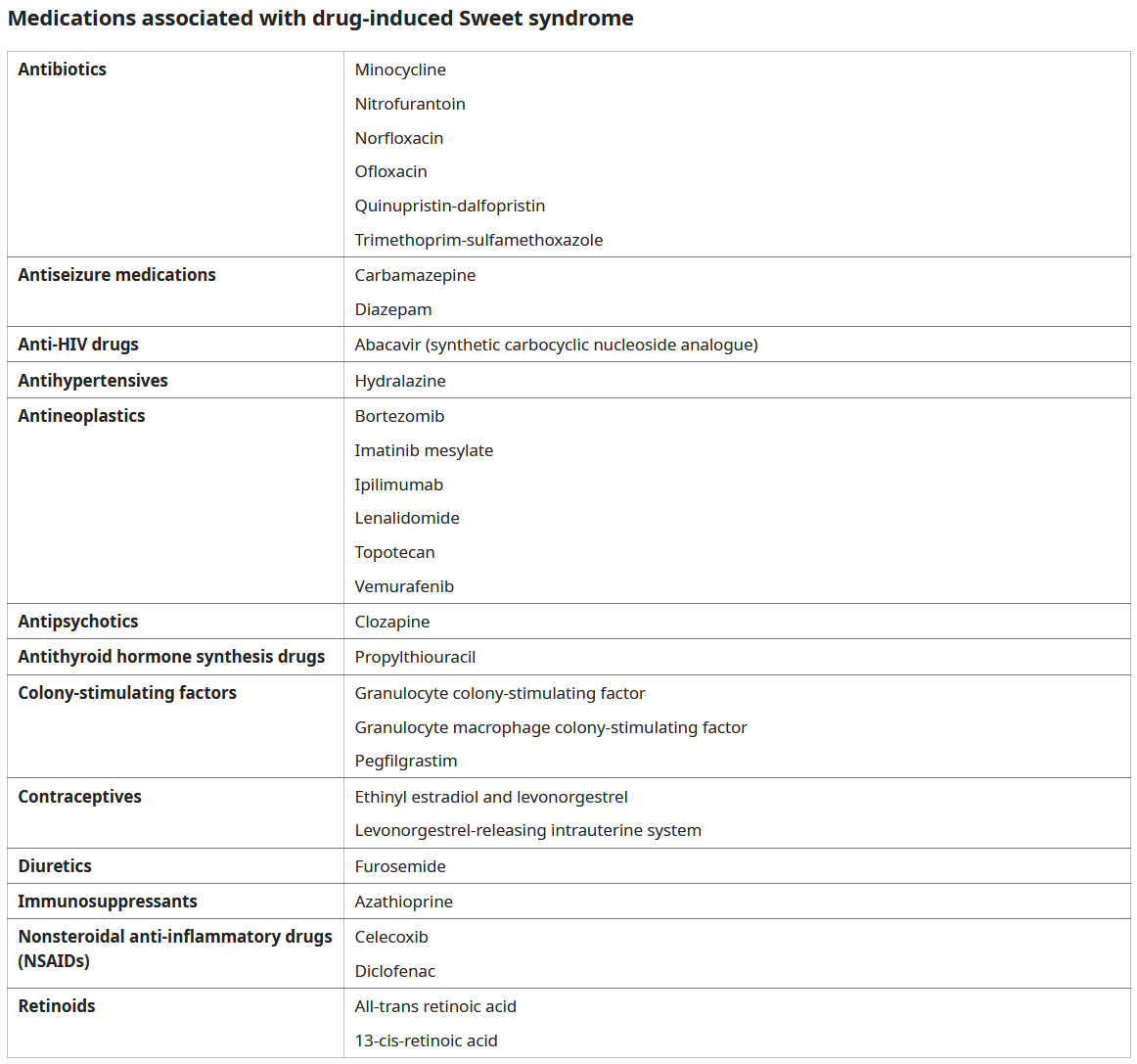
- Drug-induced: Many drugs have been implicated (most commonly G-CSF). Typically appears ~2wk after first exposure and will recur on re-exposure.
Pathophysiology :
- Not well established. Thought to be a hypersensitivity reaction to microbial, tumor, or other antigens leading to production of cytokines which recruit neutrophils
Diagnostic Testing:
- Peripheral leukocytosis with neutrophilia is present in most patients
- Non-specific inflammatory markers (ESR/CRP) are also elevated
- Two separate sets of diagnostic criteria used:
-
Classical or Malignancy associated (2 major + 2/4 minor criteria):
- Major criteria:
- Abrupt onset of painful erythematous plaques or nodules
- Histopathologic evidence of a dense neutrophilic infiltrate without evidence of leukocytoclastic vasculitis
- Minor criteria:
- Fever (>38°C)
- Association with underlying hematologic/solid malignancy, inflammatory disease or pregnancy, OR preceded by upper respiratory infection, gastrointestinal infection, or vaccination
- Excellent response to treatment with systemic glucocorticoids or potassium iodide
- Abnormal laboratory values at presentation (3/4 of: ESR >20 mm/hour, elevated CRP, >8000 leukocytes, >70 percent neutrophils)
- Major criteria:
-
Drug-induced (all 5 criteria):
- Abrupt onset of tender or painful erythematous plaques or nodules
- Dense dermal neutrophilic infiltrate without leukocytoclastic vasculitis
- Fever (>38°C)
- Temporal relationship between drug ingestion and clinical presentation, OR temporally related recurrence after oral challenge
- Temporally related resolution of lesions following drug withdrawal or treatment with systemic corticosteroids
-
Treatment :
- No high-quality data/consensus on best treatment options
- Mostly relies on systemic glucocorticoids
- Treat underlying condition: treat cancer, remove offending drug,
Prognosis:
References:
- https://www.ncbi.nlm.nih.gov/books/NBK431050/
- https://www.uptodate.com/contents/sweet-syndrome-acute-febrile-neutrophilic-dermatosis-pathogenesis-clinical-manifestations-and-diagnosis
- https://www.uptodate.com/contents/sweet-syndrome-acute-febrile-neutrophilic-dermatosis-management-and-prognosis
Created on: Sunday 06-09-2024