Thrombotic Thrombocytopenic Purpura (TTP)
Presentation :
- Often presents with GI and neurological symptoms
- Typically presents WITHOUT renal failure (unlike other MAHAs like Atypical HUS (Compliment Mediated HUS) which often have florid renal failure)
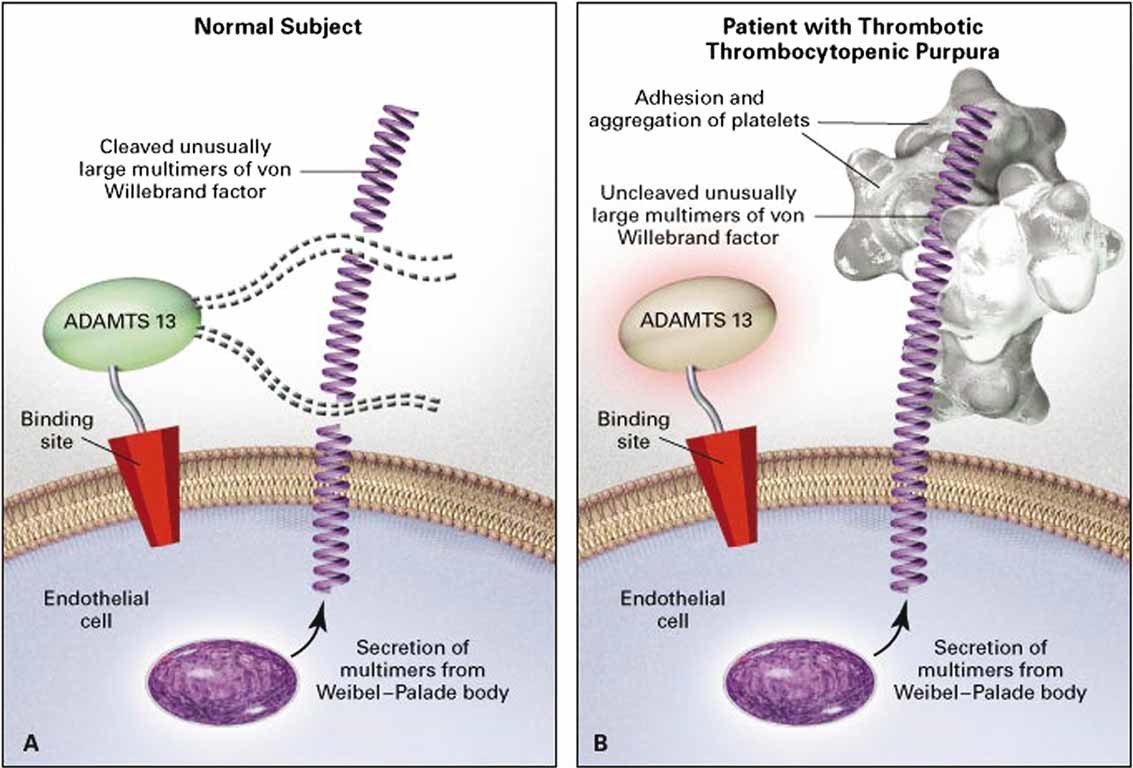
Pathophysiology :
- Deficiency of ADAMSTS13:
- Congenital: occurs typically early in life (pediatric) so less likely to be seen by IM
- Acquired: Autoantibodies inhibit ADAMSTS13 activity
- ADAMSTS13 works to cleave vWF multimers into shorter chains. When vWF gets really long they more readily bind platelets and cause thrombosis
Diagnostic Testing:
- CBC w/ smear, Coags, Fibrinogen, LDH, Haptoglobin, ADAMSTS13 level
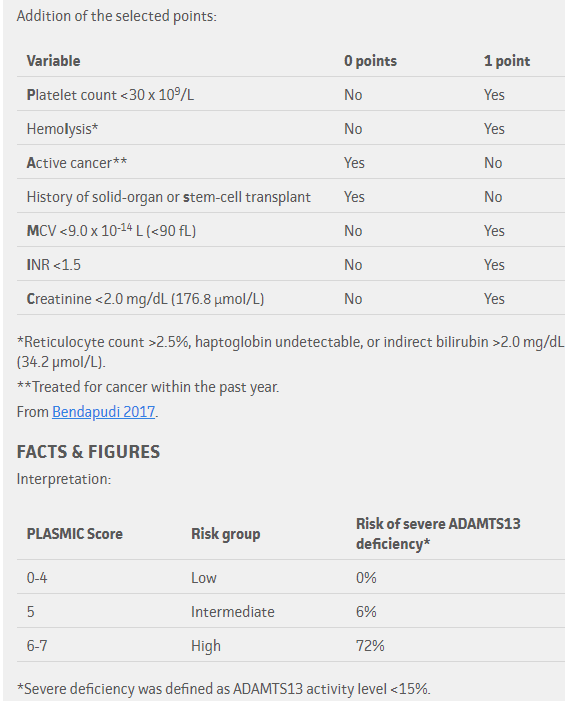
- PLASMIC score to help predict ADAMSTS13 deficiency
- ADAMSTS13 activity
Treatment :
- 1st Line Therapies:
- Plasma exchange
- Removes long-chain vWF
- Replaces ADAMSTS13
- Removes ADAMSTS13 auto-antibodies
- Corticosteroids
- Suppresses plasma cells producing anti-ADMAMSTS13 autoantibodies
- Rituximab
- Eliminates plasma cells producing anti-ADMAMSTS13 autoantibodies
- Doesn't reduce mortality but reduces # of plasma exchanges needed, duration of treatment/hospitalization, and prevents relapse
- Plasma exchange
- Bortezomib
- Can consider in treatment failure
- Caplacizumab
- Binds the A1 domain of vWF which normally binds platelets, preventing platelet aggregation
- New agent, not on all formularies
- Not clear exactly where this fits into treatment algorithms
- Transfusion
- Clinically significant bleeding is rare despite severe thrombocytopenia. Avoid platelet transfusions unless significant bleeding occurs, or an high bleed-risk procedure is required.
Prognosis:
- Very high mortality in the first 24 hours
References:
Created on: Thursday 02-15-2024