Traumatic Brain Injury (TBI)
Presentation :
- ==Mild TBI (aka concussion): typically causes temporary neurologic impairment without evidence of structural damage on conventional neuroimaging. ==
- In most patients, the physical examination is normal and diagnostic investigation is unnecessary
- Headache is consistently the most common symptom and is among the most disabling sequelae
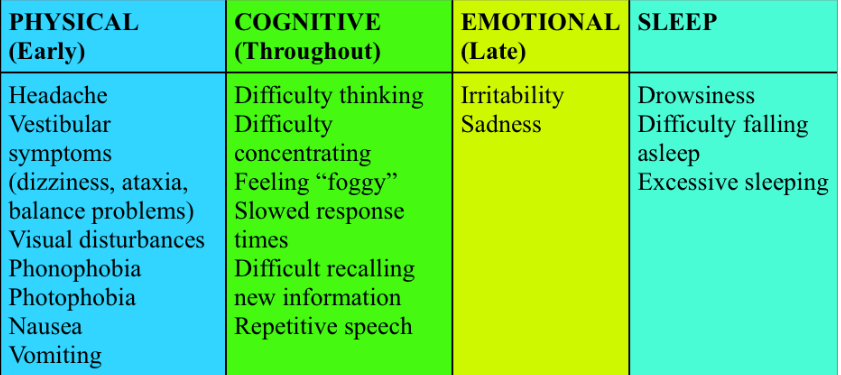
- Common TBI symptoms by domain:
- Severe TBI may present with altered consciousness, seizures, repeated vomiting, or focal neurologic deficits.
- Postconcussion syndrome describes the persistence of symptoms of mild TBI beyond a typical recovery period of several weeks.
Pathophysiology :
Diagnostic Testing:
- Patients with mild TBI, a normal neurologic examination, and (when necessary) a normal head CT scan may be safely followed as outpatients.
- CT in patients with mild TBI should be performed if any of the findings below are positive. This has a nearly 100% sensitivity but low specificity.
- Age >60 years with loss of consciousness or age ≥65 years with no loss of consciousness
- Vomiting
- Severe headache
- Posttraumatic seizure
- Drug or alcohol intoxication
- Persistent drowsiness or short-term memory deficit
- “Dangerous” mechanisms of injury (fall from height greater than 3 feet or 5 steps, ejection from a vehicle, being struck by a vehicle as a pedestrian)
- Glasgow Coma Scale score <15
- Focal neurologic deficit
- Physical evidence of open, depressed, or basilar skull fracture
- Coagulopathy
- CT in patients with mild TBI should be performed if any of the findings below are positive. This has a nearly 100% sensitivity but low specificity.
Treatment :
- Athletes suspected of having a mild TBI should be immediately removed from play and should undergo sideline assessment.
- Return to play may be considered after 1 or 2 days of physical and cognitive rest, resolution of symptoms both at rest and with exertion, and normalization of cognition.
- Postconcussion syndrome: supportive care and rehab.
- NSAIDs and triptans may be useful in treating posttraumatic headache. Tricyclic antidepressants, SSRIs, and SNRIs can also manage posttraumatic headache as well as mood and anxiety disorders.
- Ppioids and butalbital products should be avoided.
- β-Blockers, antidepressants, and antiepileptic drugs may be useful for headache prevention in patients with persistent posttraumatic headache.
- A seizure occurring within the first week of a traumatic brain event is felt to be symptomatic (closely related to neurologic or systemic insults) and does not warrant antiepileptic therapy
Prognosis:
References:
- MKSAP
Created at: periodic/daily/August/2023-08-06-Sunday